| JOURNAL 2018 |
| North Craven Heritage Trust |
Introduction
Last year Mary and Michael Slater provided a fascinating account, which appeared in this journal, of the medical practitioners who served the people of Settle from the late 17th century onwards. This inspired me to investigate the other side of the coin - the people they treated - that is the patients. What diseases afflicted the people of North Craven and what did they die of? The Slaters’ article was based mainly on information gleaned from wills and probate inventories. Although these documents provide glimpses of the people and their lives they tell us little about their health and ultimately their death.Prior to the Births and Deaths Registration Act of 1836, and the introduction of civil registration, baptisms and burials were recorded in parish registers. It is only comparatively recently, from 1845, that a doctor has had to certify the cause of death before the deceased could be buried. So we are reliant on parish registers for information from the late sixteenth century to the start of the nineteenth century. Unfortunately the registers are not always complete and in the case of Clapham parish there are obvious gaps until the early seventeenth century. For this study I have focused on Clapham but checked my findings with the neighbouring parishes of Giggleswick and Ingleton.
In the case of baptisms the parish registers usually record the name of the child, the names of the parents and the date of the baptism. Occasionally the actual date of birth was noted and where the baptism was of an adult, this too was recorded. With burials the name of the deceased and the date of burial were registered. Where the deceased was still a child or adolescent the name of one of the parents was also entered. Sometimes the age of the deceased was also noted. Accidental deaths were occasionally recorded. For example, Robert Procter was buried on 12th August 1677 and the comment was added ‘fell from a cliff in Norber’. Another rare addition was Laurence Remington ‘drowned crossing the bridge near Turnerford on 17th December (1706)’. Other information available from the registers was the abode of the person and sometimes their occupation. So the barest amount of information is available with which to attempt to reconstruct a picture of the lives of people living in the area. What makes the Clapham registers so special is that from January 1804 to December 1812, the incumbent had also recorded the cause of death. We will return to this later, but first of all what can be made of the bare records?
Infant Mortality
Infants are among the most vulnerable members of any society and are often at higher risk of dying than any other age group. So measures of infant mortality are often used as an indicator of the general health of a society and are usually expressed as the number of deaths under one year of age per thousand live births per year. In theory the parish registers provide the number of births (baptisms) in any one year and then by checking the burial records for the following twelve months an assessment of the number of deaths is reached. So for a child baptised in October 1665 the burial register has to be checked until October 1666. This is a very time-consuming task! It was therefore decided to sample one year per decade from 1615 to 1815 and the results are shown in Figure 1. There appears to have been an increase in mortality at the start of the seventeenth century, reaching a peak in 1665 (228 burials), and then declining at the end of the period. However, the graph is very spikey with considerable variation between annual mortality rates. In England the national infant mortality rates have been calculated to have been about 175 per 1000 live births in 1581, increasing to about 200 by the late 17th century and then decreasing to approximately 150 by the early 19th century. The pattern is not too dissimilar for Clapham though the peak was slightly earlier. All of these figures are considerably higher than those reported more recently. According to the Office for National Statistics the infant mortality rate for 2016 was 3.6.So how reliable are the figures calculated for Clapham? Fortunately in the registers for 1805 and 1815 the date of birth as well as baptism were recorded. It is clear that in some cases there was a delay of several weeks between birth and baptism: so for any calendar year the baptism records would include children born the previous year and exclude others born in that year but not baptised until the following year. On the whole these two should balance each other. Perhaps more significant was the discovery that in each of these sample years there were three children who were recorded in the burial register but had not been baptised. With the appropriate adjustments the mortality rate for 1805 rose from 47 to 109 per thousand and for 1815 it rose from 97 to 138. These large increases are due to the small numbers in the sample. Clearly the rates calculated for Clapham are significantly lower than the actual level of infant deaths.
In theory it would be possible to calculate childhood mortality rates, or the deaths of children below the age of five years. In the 75 years between 1556 and 1652 a total of 5307 children were born in the Swaledale parish of Richmond. Of these 1348 (25%) died before the age of five years [Fieldhouse & Jennings, 1978].
Birth and Death Rates
Unfortunately we do not have reliable estimates of the size of the population for Clapham as the national censuses were not introduced until the 19th century. Thus it is not possible to calculate the birth and death rates (the births and deaths per 1000 people). However it is possible to count the number of births and deaths from the registers. Figure 2 shows the total figures for each decade. For each decade the number of births exceeded the number of deaths, so without migration the population of Clapham would have increased throughout the period. What is also evident is that there was considerable variation in the number of deaths. This is even more apparent when individual years are considered. In the 17th and 18th centuries Europe was subject to periodic surges in the number of deaths, due to epidemics of infectious diseases or short-term famines. These peaks in the number of deaths are often referred to as ‘mortality crises’. These peaks have been identified by comparing the number of burials in each year with that expected in an ‘average’ year. As the average may change with the rise or fall of a population a ‘moving’ average is often used. For example for the year 1700 the number of burials is compared with the average for 1695 to 1705. Then for 1701 the number of burials is compared with the average for 1696 to 1706. So how much higher do the deaths have to be above the average to be recognised as a crisis year? Some historians use a figure of twice whilst others use a factor of one and a half depending on the size of the parish.In the former case (twice the ‘moving’ average) none of the years in the period for Clapham would be classed as a crisis year. When the factor of one and a half was used the following years could be classed as having significantly higher mortality: 1623, 1624, 1655, 1729, 1741, 1742, 1775 and 1791. Is it possible to find out more about the causes of this high mortality? Was it due to food shortage and famine or was it caused by epidemics of infectious disease? Is it possible to speculate which diseases were involved? To answer these questions involves a more detailed, monthly, analysis of the number of burials and comparisons with neighbouring parishes.
The Crisis of 1623
In many parts of northern England this year was marked by a severe mortality crisis. A study of nine Cumbrian parishes provided convincing evidence that not only was there a harvest failure but the resulting famine resulted in an increase in deaths [Appleby, 1973]. Likewise there was an increase in mortality in Dentdale though it was concluded that a combination of factors may have been to blame. In other words malnutrition may have rendered the population vulnerable to unspecified infectious diseases [Stacey, 2000]. A study of mid-Wharfedale parishes demonstrated an increase in mortality but it was not as high as seen elsewhere [Long and Pickles, 1986]. Although the harvest may have been no better than in the rest of the region it was suggested that easy access to markets for the sale of livestock and the existence of secondary industrial activities may have enabled people to buy food and avoid starvation.Figure 3 shows the number of deaths for the parishes of Clapham, Giggleswick and Ingleton. In Clapham the first peak in mortality appeared in June and July 1623 when nine and eight burials were recorded respectively (compared to an average of less than two per month). A second peak occurred in December 1623 (nine burials) which steadily declined until April 1624 (five burials), followed by an average of just over two per month to December of that year. This would not appear to fit the pattern expected if famine was the cause of the mortality.
In Ingleton there was no peak in the summer of 1623, but like Clapham there was an increase in burials in the autumn until April 1624. At its height there were 11 burials per month which fell to an average of just over one per month. Again the pattern does not fit that expected from a harvest failure. For Giggleswick there was a peak in deaths in March and April 1623 (12 and 14 burials) followed by a further one in August (13 burials). These were followed by a period of sustained mortality from October 1623 to March 1624 which then fell to an average of just under three burials per month. The pattern was similar to that observed in Clapham but the autumn to spring crisis lasted longer. Another aspect to consider is the balance between adult and child/adolescent burials. For the prolonged peak in Clapham 30 adults were buried compared to seven children. For Ingleton the difference was less stark: 26 adults and 18 children. This was also the case in Giggleswick (29 adult and 21 child burials).
It is generally assumed that where there has been a failure in the harvest the number of deaths would start to increase from September and would continue to the next harvest the following August. If there were reserves in storage then the famine might be delayed for all but the poorest members of the community. This might explain the delay in the peak mortality to the end of the autumn 1623 in Clapham and Ingleton. Even so one would have expected the crisis to last longer to the summer of 1624 but this was not the case. Perhaps all three parishes had access to grain from outside the area. It is also assumed that in cases of famine there would be more deaths of children compared to adults but this was not seen in any of the three parishes.
A final aspect to consider is the impact on the number of births. Famine is known to disrupt the menstrual cycle with a resulting decline in the number of births. All three parishes showed a steep fall in the number of baptisms in 1623 with a further fall in 1624 (apart from Ingleton). The number of baptisms recovered in 1625 but not consistently to the same level as seen in 1622. For example, In Clapham there were 42 baptisms in 1622, which fell to 24 and 17 for the next two years and then recovered to 39 in 1625. If famine was the cause of this decline in the number of births then one would expect the fall to occur in 1624 because of the nine month time-lapse, and yet the decline had started the previous year.
The Crisis of 1729
The years 1727 to 1730 were supposedly the second worst crisis between 1541 and 1871. Mortality was particularly high in northern England and although the harvests of 1727 and 1728 seem to have been poor the crisis does not appear to have been a result of famine. It has also been suggested that the crisis was more severe in the countryside rather than urban areas and that the poor and elderly were particularly affected [Healey, 2008].Using the ‘moving’ average method only 1729 would be classed as a crisis year for Clapham. The average number of burials from 1722 to 1726 was 28 per year. The number then rose to 43 (1727 and 1728), 56 (1729) and 52 (1730). The average for the following five years fell to 28 per year. In other words there were four years of higher than expected mortality which suggests that there were several causes for the increased number of deaths: possibly a combination of famine and outbreaks of several infectious diseases.
Figure 4 shows the monthly burials for Clapham, Giggleswick and Ingleton. For Clapham there was a peak starting in December 1728 which lasted until April 1729. There was a similar peak in Giggleswick but of shorter duration (from March to May 1729). In Ingleton there were two peaks, one in January and the other in March 1729. In Giggleswick the majority of burials were of adults (29 adults, 10 children). The contrast was even more striking in Clapham where 43 adults and 6 children died. In Ingleton there were 12 adults and 9 children buried. All three parishes showed further peaks in mortality in the late winter or early spring of 1730.
Focusing on the 1729 crisis is it possible to identify the possible causes based on the timing and the impact on different age groups? It appears unlikely to have been caused by starvation due to the duration and timing of the deaths. Of the infectious diseases it is possible to rule out measles, scarlet fever, whooping cough and dysentery as these primarily affected children or tended to appear in the late summer. Although smallpox spreads slowly it only affects those who were not exposed to the virus since the last outbreak, i.e. mainly adolescents and children. Influenza is generally a winter disease and any epidemic tends to run its course in about seven weeks. Again this does not seem to fit the pattern recorded for 1729 (but does match that observed for the following year). Consumption (tuberculosis) can also be excluded as it is a chronic condition with deaths occurring throughout the year. The first case of cholera appeared in Sunderland in 1831 so this too can be ruled out. This leaves the possibility of typhus fever or typhoid.
In the eighteenth century these two diseases were lumped together under the term ‘continuing fevers’ to distinguish them from the ‘intermittent fevers’ such as is produced by malaria. It was not until the next century that physicians were able to differentiate between typhus and typhoid. Both were characterised by fever and a blotchy pink rash: one tended to be acute, killing within days (typhus), whilst the other was chronic, sometimes resulting in months of sickness (typhoid). The cause of these diseases had to wait until the early years of the twentieth century. Typhus is caused by a bacterium transmitted by an infected body louse. Typhoid is a water borne disease caused by human excreta leaking into the water supply or by the consumption of contaminated food. Of course it is pure speculation as to which of these diseases or neither was responsible for the peak in mortality. The season would suggest typhus, due to the reluctance to wash during the cold winter months. Also the dispersed geographical nature of the deaths might suggest that it was not due to typhoid fever. It is unlikely that we will ever discover the cause!
Causes of Death 1804 - 1812
During this period there were 324 burials in the parish of Clapham and of these only 14 did not have a cause of death entered in the register. The most frequently stated cause was ‘infirmity’ (30%) which was generally associated with the older part of the population. Likewise ‘weakness’ (8%) was predominantly associated with infant mortality. Other terms, such as ‘fever’ and ‘convulsions’, are more a description of the symptoms rather than the disease involved (11%). Nevertheless there is an interesting array recorded. The greatest killer was consumption (19%) compared to smallpox, which accounted for 3% of deaths. There are a large range of causes listed: accidents (3% which included broken leg and dislocation of the hip), chin cough (whooping cough, three cases), cancer (two cases), gravel and stone (kidney/bladder stones, three cases). There were just two deaths attributed to childbirth and just one of scarlet fever. The latter is a reminder that this disease appeared in a mild form in the 18th century and again in the present day but became a major childhood killer for much of the 19th century. There was just the single death attributed to typhus fever although some 14 people died of unspecified fever.This raises the question of who diagnosed the cause of death. Was it the incumbent or the relatives of the deceased? Perhaps the local apothecary or surgeon was consulted. Some of the causes are vague (cramp in the stomach) whilst others (internal impostume) suggest some medical knowledge but are equally imprecise.
In 1808 there was an outbreak of smallpox in the parish of Clapham. The first burial was in the middle of March, who was also the oldest victim, aged 15 years. There were a further nine burials, all children. The last one was of Charles Hudson in September. His older brother had died of the same disease the previous month. So of the 49 burials that year ten were due to smallpox and yet this was not a crisis year. As we know the age of the oldest victim it is possible to calculate the number of births in the previous 16 years and subtract the number of childhood deaths for the same period. This provides a childhood population of 553 in Clapham in 1808. As there were ten deaths from smallpox this provides a mortality rate of 1.8% of the childhood population. One of the features of smallpox is that once one has been exposed to it one has immunity to further outbreaks. This would suggest that the previous outbreak was at least 15 years (the age of the oldest victim) prior to 1808. The parish records show that 1791 was a crisis year with some 67 burials, 37 of which were of children under the age of 18 years. This suggests that there may have been an outbreak of smallpox in 1791.
Unlike smallpox the burials for people suffering from consumption appeared throughout the period 1804 to 1812. The number of burials ranged from one to twelve each year with an average of six per year. The age of the victims ranged from under a year in age to 74. The average age at death for women was 29 years whilst the average for men was 35 years. Although the cause of the disease was not known at the time it was recognised that sleeping in close proximity to a person who showed the symptoms was to be avoided [Buchan, 1781]. The danger of close contact is illustrated by the Redmayne family in Clapham. Robert, aged five months, was buried in February 1811. His mother, Catherine, died in April. Her daughter, Alice, was buried in June 1812, at the age of 6 years. Catherine’s husband, and the children’s father, Robert Redmayne, was buried in July 1812. In each case the cause of death was ascribed to consumption.
Discussion
Anyone who has used parish records for historical research soon realises that these registers are far from perfect. Nevertheless, they provide important demographic information for the period before the introduction of civil registration. Analysis of baptismal and burial records can provide some interesting insights into the diseases and causes of death in the early modern period. The data show that there was considerable variation in birth and mortality rates over the period. This variation was also reflected in the levels of infant mortality. Detailed analysis of the ‘crisis years’ of 1623 and 1729 also demonstrates that there was significant variation between neighbouring parishes in North Craven. Although it is tempting to speculate as to the causes of these peaks in mortality it is rarely possible to attribute them to a single cause.The early 19th century records of the causes of death for the Clapham parish are rare and fascinating. In many instances the cause of death was not known: there was still confusion between the symptoms and the cause of these symptoms. Deaths resulted from accidents, complications of child-birth, cancer as well as a multitude of infections. Some of these diseases were endemic in the population, developing over years, such as consumption. Others occurred in epidemics, such as smallpox, which spread rapidly through these rural communities.
The stark records of the Redmaynes highlight the impact of disease on individual families. It is not difficult to imagine the misery and suffering from the simple statistics. Contemporary letters and journals provide further details. In 1794 a Lancashire gentleman, Richard Hodgkinson, visited his friends (the Flavel family) and noted the loss of three of the children. He wrote ‘But the burial of three children all of the same disorder has been so severe a stroke upon Mrs Flavel that she is quite dispirited and seems apprehensive of living to bury the other three’ [Wood, 1992].
Although there had been advances in the understanding of human anatomy and physiology, medical knowledge at the end of 18th century was still very rudimentary. William Buchan’s Domestic Medicine was a popular book which had reached the seventh edition by 1781. Aimed at the self-help market, rather than the medical profession, it highlights the confusion about the causes of diseases and their treatment. For example, he distinguished between several different forms of fever: putrid or spotted, military, remitting and intermitting or ague. In each case he prescribed Peruvian bark as a treatment. In fact we now know that Peruvian bark, as a source of quinine, is only effective in the prevention of malaria or intermitting fever. Buchan’s suggested treatment of malaria was initially to cleanse the stomach and bowels with a purging medicine. If this did not result in a cure then bleeding was recommended and if this did not work then Peruvian bark was prescribed. Not only were many of the treatments ineffective but many were even harmful.
For those who found such books too confusing or the treatments ineffective there was professional help at hand. Those with resources could turn to the physicians, surgeons and apothecaries. The account book of Roger Strickland of Richmond contains numerous entries relating to the care of his children. In 1748 he paid Dr Assque and Mr Wayne, an apothecary, a total of Ł15-9s-10d. The following year the bill totalled Ł7-14s-6d. Unfortunately there is no evidence that their treatment was any more successful.
Despite high levels of infant and childhood mortality there were some who survived to old age. Richard Hodgkinson described how on a visit to Manchester in 1844 he found he was unable to stand from the excessive pain in his left leg. Having been examined by two surgeons they “immediately bled me by cupping between my shoulders. At the end of seven weeks I could walk about the room and in ten weeks I could walk a little in the garden”. He continued “This attack has not seriously injured my bodily health but it seems to be rather hastening the feebleness of old age. I have completed my eightieth year”.
The major advances in the control of infectious diseases had to wait until later in the 19th century with the provision of effective sanitation and clean drinking water. This was followed in the 20th century by the medical advances that today we take for granted.
References
- Appleby, A. B., 1973. Disease or Famine? Mortality in Cumberland & Westmorland 1580-1640. Economic History Review 26: 403-432
- Buchan, W., 1781. Domestic medicine: or, a treatise on the prevention and cure of diseases by regimen and simple medicines. London: Strahan
- Fieldhouse, R. and Jennings, B., 1978. A history of Richmond and Swaledale. London: Phillimore
- Healey, J., 2008. Socially selective mortality during the population crisis of 1727-1730: evidence from Lancashire. Local Population Studies 81: 58-74
- Long, M. and Pickles, M., 1986. An inquiry into mortality in some mid-Wharfedale parishes in 1623. Local Population Studies 37: 19-35
- Stacey, F., 2000. Deadly days in Stuart Dentdale. Sedbergh Historian IV: 8-11
- Turner, M. and Summerbridge Tutorial Group, 1995. Kith and kin: Nidderdale families 1500-1750. Summerbridge Tutorial Group
- Wenham, L. P., 1982.Roger Strickland of Richmond 1680-1749. North Yorkshire County Records Office.
- Wood, F. and K., 1992. A Lancashire gentleman. The letters and journals of Richard Hodgkinson 1765-1847. Stroud: Sutton
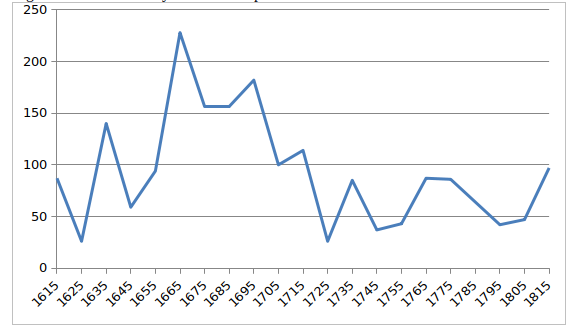
Figure 1 Infant mortality rates for Clapham
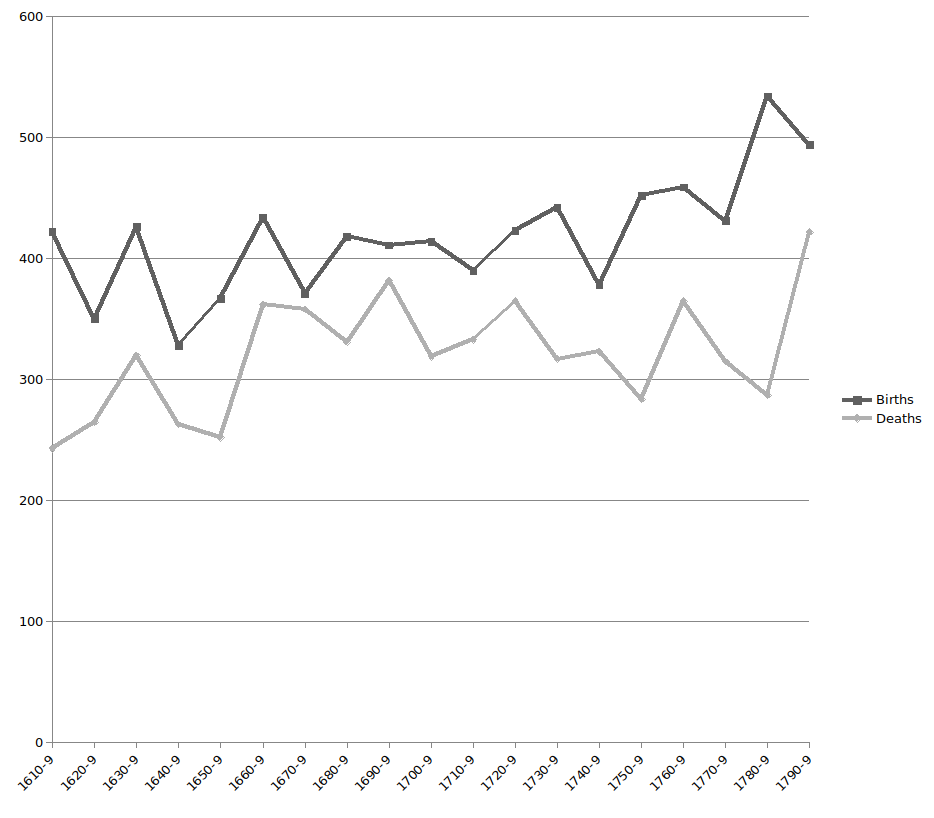
Figure 2 Clapham: Total figures for each decade

Figure 3 Number of deaths for Clapham, Ingleton and Giggleswick
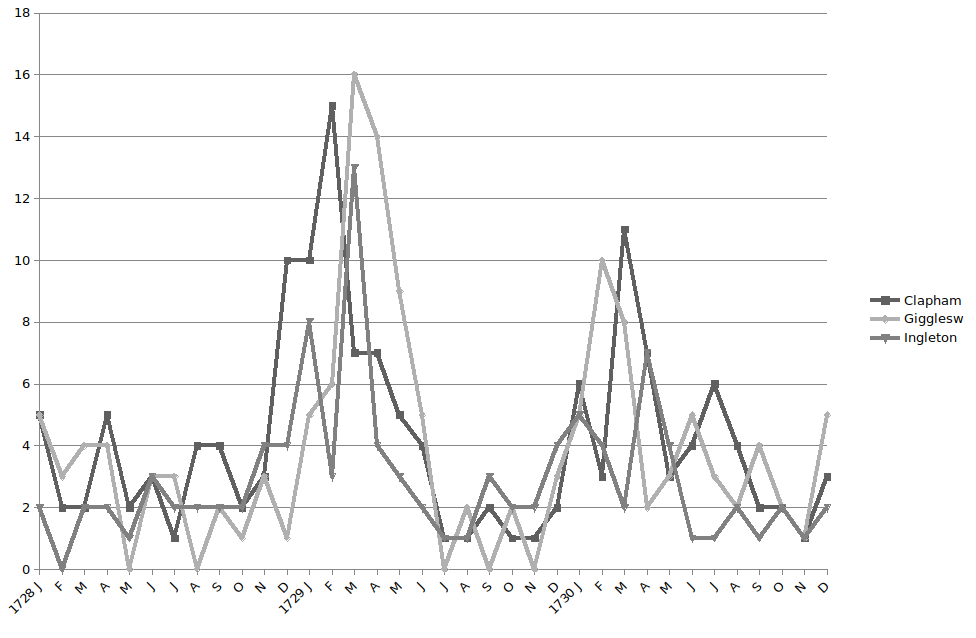
Figure 4 Monthly burrials for Clapham, Ingleton and Giggleswick